

The Quiet End of Sixteen Thousand Canadians
New federal data reveals how assisted death has moved from a contentious legal battlefield to a stable medical reality for the terminally ill.

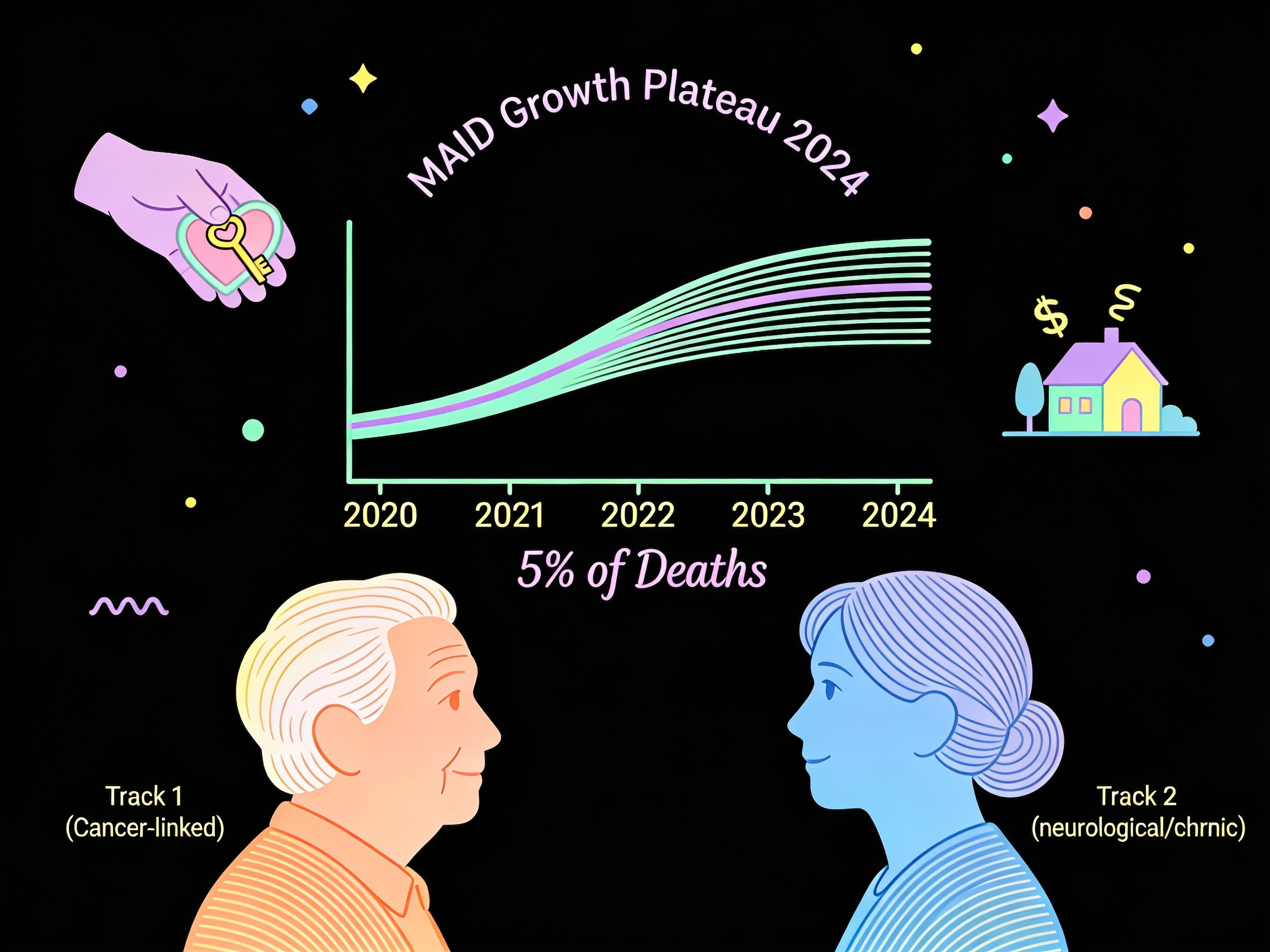
It began as a roar of legislative debate in Ottawa, but by 2024, Medical Assistance in Dying had settled into a quieter, more bureaucratic rhythm within the Canadian healthcare system. The sheer novelty of the law has faded, replaced by the stark logistical reality of end-of-life care in a nation with an aging population. According to the federal government’s latest comprehensive review, 16,499 individuals chose to end their lives through this legal framework last year. It is a number that represents the population of a small town, yet the data suggests the explosive growth of previous years is finally beginning to plateau.
The hysteria that once predicted a runaway train of assisted deaths has been tempered by the cold hard facts of the sixth annual report. While the total number of provisions rose, the rate of increase has slowed dramatically. In 2020, the growth rate surged by nearly thirty-seven percent year over year. In 2024, that growth dropped to just under seven percent. The curve is flattening. Medical Assistance in Dying now accounts for just over five percent of all deaths in Canada, a statistic that places the nation in line with other jurisdictions where similar laws have matured.
Behind these aggregate numbers lies a complex tapestry of human suffering and autonomy. The report does not just tally deaths; it profiles the dying. It reveals who they are, where they live, and perhaps most importantly, why they chose to leave. The prevailing narrative that the system targets the marginalized or the economically destitute is being challenged by the government’s own socio-economic analysis. The people accessing this service are not typically the ones falling through the cracks of the social safety net. They are, by and large, the elderly and the terminally ill who are staring down the barrel of a predictable and agonizing end.
The Fever Break
For years, critics and proponents alike watched the ascending graph of MAID deaths with bated breath. The exponential rise in the early years of legalization provided ammunition for those who feared a slippery slope, where the option to die would become a compulsion. However, the 2024 data indicates that the system is reaching a saturation point relative to the population. The frenetic pace of adoption has broken.
This stabilization is occurring primarily within the largest cohort of recipients: those whose natural death is reasonably foreseeable. Known in the legal parlance as Track 1, these individuals make up the overwhelming majority—nearly ninety-six percent—of all cases. These are not patients making a choice between a long life and a quick death. They are patients choosing between a painful death now or a painful death weeks from now.
The demographics of this group paint a clear picture of the Canadian mortality landscape. The median age is seventy-eight. They are our parents and grandparents. Cancer remains the great driver of these decisions, accounting for nearly sixty-four percent of all Track 1 cases. As the leading cause of death in the country, cancer brings with it a specific trajectory of decline—loss of autonomy, increasing pain, and the slow erosion of bodily function—that aligns closely with the eligibility criteria for assisted death.
The data suggests that the integration of MAID into the healthcare system has normalized. It is no longer a fringe option sought by the few, but a standard consideration in palliative discussions. This normalization is reflected in the outcome of the requests themselves. While over twenty-two thousand written requests were submitted in 2024, not all resulted in a provision. Thousands of applicants died naturally before the procedure could take place, a tragic bureaucratic footnote that speaks to the fragility of the applicants. These were people racing against their own biology, and in nearly four thousand cases, biology won.
A Tale of Two Dying Trajectories
While the vast majority of cases involve terminal illness, the spotlight often falls on the small minority of applicants whose death is not reasonably foreseeable. This category, known as Track 2, was introduced following legislative amendments in 2021 and represents a fundamental shift in how the law is applied. It allows those with chronic, enduring, and intolerable suffering to access relief even if their condition is not immediately fatal.
In 2024, Track 2 provisions accounted for only 4.4 percent of the total, yet this group looks distinct from the general MAID population. They are younger, with a median age of roughly seventy-six, and they are significantly more likely to be women. While men slightly outnumber women in the terminal Track 1 category, women make up nearly fifty-seven percent of Track 2 cases.
This gender divide mirrors broader epidemiological trends. Women in Canada statistically live longer than men but are also more likely to live those later years with chronic, debilitating conditions. They are the survivors of acute illness who are left to manage the long tail of disability. The report indicates that neurological conditions and “other” chronic issues like frailty, chronic pain, and autoimmune disorders are the primary drivers for this group.
These individuals also traverse a much longer road to access the procedure. The safeguards for Track 2 are more rigorous, requiring a minimum ninety-day assessment period to ensure that the request is not a fleeting reaction to a temporary crisis. The data confirms that practitioners are taking this seriously. The median time between a request and provision for Track 2 patients was 118 days, compared to just fifteen days for those who were terminally ill. Some assessments stretched on for over a year, suggesting a cautious approach by clinicians navigating complex medical and ethical terrain.
The suffering described by these two groups also diverges. While both cite the loss of ability to engage in meaningful activities as a primary grievance, Track 2 recipients were far more likely to report isolation, loneliness, and a loss of dignity. They are living with conditions that do not kill them quickly but slowly strip away their connection to the world and their sense of self.
Dispelling the Myth of the Economic Victim
One of the most persistent fears surrounding Canada’s assisted dying laws is the specter of coercion born of poverty. The argument posits that vulnerable Canadians, unable to afford proper care or housing, might be driven to seek death as a solution to economic deprivation. The federal government attempted to answer this charge by linking MAID data with neighborhood income quintiles and indices of marginalization.
The results contradict the dystopian narrative. The analysis found that people receiving MAID do not disproportionately come from the lowest income neighborhoods. In fact, under Track 1, recipients were slightly less likely to be in the lowest income bracket compared to the general population of dying Canadians. Conversely, there was a slightly higher representation of MAID recipients in the highest income quintiles.
This trend holds when looking at measures of marginalization such as “economic dependency” and “situational vulnerability.” Across both tracks, MAID recipients generally lived in neighborhoods that were less deprived than the average Canadian decedent. This suggests that access to MAID functions much like access to other specialized healthcare services in Canada: it is navigated more easily by those with the social capital and stability to advocate for themselves.
However, there is a nuance in the Track 2 data that warrants attention. While they are not overwhelmingly poor, Track 2 recipients are more likely to live alone and reside in areas characterized by “residential instability.” Forty-one percent of Track 2 recipients lived alone, compared to thirty-two percent of Track 1 recipients. This aligns with the higher reports of loneliness and isolation within this group. It paints a picture not of economic destitution, but of social atomization—people managing chronic suffering in solitude, without the buffer of a family unit to absorb the daily burdens of their illness.
The Silence in the Statistics
While the socio-economic data is robust, the report reveals significant gaps in our understanding of race and Indigenous identity within the MAID system. 2024 marked the second year of mandatory data collection on these demographics, yet the picture remains incomplete due to varied collection methods across provinces and the inherent difficulties of self-identification.
The vast majority of those who chose to answer the race-based questions identified as Caucasian. Over ninety-five percent of recipients were white, a number that far exceeds the demographic makeup of the country. This homogeneity suggests that racialized communities are accessing MAID at significantly lower rates. Whether this is due to cultural views on death, a lack of access to the system, or a deep-seated mistrust of healthcare institutions remains an open question.
The data on Indigenous peoples is particularly fraught. Only 164 people self-identified as First Nations, Métis, or Inuit, representing roughly one percent of all MAID provisions. When compared to the proportion of Indigenous people in the general mortality statistics, this is a massive underrepresentation. In the territories, where Indigenous populations are highest, the gap is stark.
Federal officials suggest this discrepancy could stem from a variety of factors, including the remoteness of communities, the historical trauma inflicted by the medical system, and distinct cultural worldviews regarding end-of-life choices. The report notes that Indigenous partners have called for caution in interpreting this data, emphasizing that the “silence” in the numbers may speak louder than the numbers themselves. It reflects a healthcare system that has not yet built the necessary trust to engage fully with Indigenous communities on the most sensitive of topics.
Care at the Edge of Life
A central pillar of the debate around MAID is the availability of palliative care. Critics have long argued that assisted dying should not be a substitute for proper symptom management and comfort care. The 2024 report provides strong evidence that the two systems are working in tandem rather than in opposition.
Nearly three-quarters of all MAID recipients received palliative care services prior to their death. For those with terminal cancer, that number rose to over eighty-seven percent. The narrative that patients are choosing death because they cannot get pain relief is not supported by the aggregate data. In fact, of the small percentage who did not receive palliative care, the vast majority did not require it or had access to it but chose not to engage with it. Only a fraction of one percent of cases involved individuals who required palliative care but could not access it.
However, the nature of the care differs significantly between the two tracks. While terminal patients accessed standard palliative services like pain management, Track 2 patients utilized a broader array of supports. They were far more likely to use physiotherapy, occupational therapy, and mental health counseling. This reflects the reality of their conditions; they were not dying of organ failure but were living with functional decline.
For Track 2 applicants, the law mandates that they be informed of all available means to relieve their suffering, including disability support services. The data shows that nearly forty-six percent of Track 2 recipients received disability supports, compared to thirty-two percent of Track 1 recipients. Yet, despite these interventions, the suffering remained intolerable to the individual. This finding reinforces the complexity of the decision. Access to support does not guarantee the alleviation of suffering, and for thousands of Canadians, the availability of care was not enough to outweigh the burden of their illness.
The Human Factor in the Machinery
The machinery of death requires operators. In 2024, there were 2,266 unique practitioners—physicians and nurse practitioners—who administered MAID across the country. This workforce has developed its own internal stratification. The majority of practitioners are family doctors, followed by palliative care specialists. This indicates that MAID remains largely a primary care issue, handled by the clinicians who know the patients best.
Interestingly, the workload is heavily concentrated. A small cadre of fewer than five percent of practitioners performed over thirty-seven percent of all procedures. These high-volume providers are likely part of dedicated MAID teams or coordination services in urban centers. Conversely, for Track 2 cases, the majority of providers performed the procedure only once. This suggests that complex chronic cases are often handled as exceptions rather than routine practice, perhaps requiring a level of specific engagement that generalists cannot sustain at scale.
The report also highlights the friction between personal conscience and professional duty. Over thirteen hundred transfers of care occurred in 2024, many necessitated by institutional policies. In provinces like Alberta and Manitoba, the majority of patient transfers were due to facilities—often faith-based—refusing to allow the procedure on their premises. This logistical hurdle adds a layer of complexity for patients who are often too frail to be moved easily, forcing them to leave their beds to exercise their federal right to die.
A Settled Law
The 2024 report serves as a barometer for a profound social change. In less than a decade, Canada has gone from a total prohibition on assisted death to a system that facilitates the end of life for over sixteen thousand citizens annually. The stabilization of the numbers suggests that the pent-up demand from the pre-legalization era has been met, and the country is now seeing the natural baseline of need.
The fears of a runaway system preying on the poor have not materialized in the data. Instead, what has emerged is a system utilized primarily by the elderly and the privileged, those with the agency to navigate a complex bureaucratic process to assert control over their final days. The rising numbers of Track 2 cases, while still small, point to a growing recognition of chronic suffering as a valid reason to exit, a shift that challenges the traditional medical definition of what it means to be “dying.”
As the government prepares for the future—including the looming and contentious question of eligibility for those with mental illness as a sole underlying condition—this report provides the baseline. It documents a system that is functioning as designed, with rigorous safeguards that slow down the process for the non-terminal while expediting it for those at death’s door. It is a system of lists, checks, and balances, but ultimately, it is a system of exits. And for 16,499 Canadians last year, it was the door they chose to open.
Source Documents
Health Canada. (2025). Sixth Annual Report on Medical Assistance in Dying in Canada 2024. Government of Canada.
Two acquaintances of mine chose MAID in 2024: a woman of about 80 who would have been considered Track 1, and a man of 60 in the Track 2 category. As a cancer survivor, although I have seen others make the choice between long-term decline and suffering and a dignified end of life, I know that this can only be a personal choice at the time and under the unique circumstances inherent to the situation. I’m grateful that Canadians have this ability enshrined in law.